Elliot Brennan writes about the modest improvements to key public health measures and policy in Myanmar.
This post is part of Tea Circle’s “2018 Year in Review” series, which looks back at developments in different fields over the last year.
There have been some clear successes made in public health in Myanmar over the past year. The release of several reports, including on public health data between 2014-2016 and the National Health Plan 2017-2021, shed light on the state of public health in the country. The following Year in Review post explores some of these achievements in the past year but also highlights the slow pace of reform.
As highlighted in April by a fire in a refuse dump in Yangon, which hospitalised dozens of people, pollution is a major health concern. Most recent available WHO data from 2012 found that a whopping 128.2 per 100,000 deaths were attributed to household and ambient air pollution in Myanmar (by contrast in North America and Europe, this crude figure was 47 per 100,000). The PM 10 level has increased in the past three years in Yangon. Hazardous waste, including hospital waste, continues to be burnt in open air urban environments. Alive, albeit late, to the problem, the government is attempting to correct this, such as through building appropriate waste incineration facilities. Indeed, the February 2018 report on Environmental Health in Myanmar by the Department of Public Health shows that there is increased attention to the issue including through new international cooperation, workshops and trainings to improve, in particular hazardous waste management but environmental health more broadly. But as the slow response to the refuse fire in April demonstrates, the sense of urgency that environmental health crises should provoke is lacking.
As I noted in a post late last year, the government’s reaction to public concern about H1N1 cases across the country in July and August highlighted just how far the government has come in acknowledging the importance of health communication and cooperation. Faced with increasing panic, the government began releasing daily updates to inform the public of the H1N1 outbreak. It is easy to play down such an achievement, but without it such incidents can very quickly spiral into mass panic and challenge disease control measures. This is contrasted with the lacklustre response in communicating the severity of the refuse dump fire. The government’s emergent crisis communication efforts in the past year showed improvement but remained uneven and underdeveloped.
Last year, a global commitment was renewed to eradicate neglected tropical diseases (NTDs). These commitments have been spurred by a strong commitment by the BRICS bloc of countries as well as significant funding from aid agencies and private sector organisations. That funding has been a boon for Myanmar where 2015 figures showed that 41 million people were at risk of infection by at least one NTD.
The WHO’s list of NTDs which includes rabies, lymphatic filariasis, soil-transmitted helminthiases, all prevalent in Myanmar, was recently enlarged to include snakebite envenoming and other diseases of concern for the country. Eradication of NTDs in other developing countries has proven tremendously successful. The Economist last year highlighted the benefits of tackling NTDs: “each dollar spent on the control of lymphatic filariasis in China, or Chagas in Brazil, has been estimated to produce benefits of $15 and $17 respectively, by reducing spending on treatment and cutting the number of prematurely curtailed working lives.” The economic argument for Myanmar to tackle NTDs, and more generally elevating public health issues as a top order priority, is clear.
That message seems to be getting through. In January 2018, the government announced K663 million for an elephantiasis (the most advanced-stage of lymphatic filariasis) eradication scheme. Another project tackling NTDs, supported by the Australian government and various universities, is creating anti-venom for the country’s deadly snake populations. This is a boon for those working in agriculture, the majority of the population, who are most at risk of snake bite. Amongst these efforts in the past year, the government and NGOs have doubled down on efforts to improve mapping of NTD hotspots, supported by the WHO’s Regional Strategic Plan for Integrated NTD control in South-East Asia Region. Action on these fronts has largely been spurred by the significant funding to combat NTDs and has been carried out by international organisations, rather than the government itself, but its benefit throughout the country will be great.
Some positive steps were made in mental health awareness in the past year. In 2014, the WHO noted that only 4,760 people had been trained in mental health care. There are only two mental health hospitals in Myanmar, with many of those beds and those of mental health wards in other hospitals occupied by long term patients, thus limiting capacity to support short term patients. The majority of those requiring mental health care fall through the gaps. As the head of psychiatry at Yangon University noted, in 2016, there was one psychiatrist per 260,000 population. That is even more concerning given the country’s traumatic past and the burgeoning drug epidemic. Myanmar now appears to be on the cusp of turning a corner in improving mental health legislation, awareness and related policy.
At the front end of improvement in mental health outcomes in the country is the promotion of mental health awareness. A good example of this in 2017 was the creation of a Facebook page called ‘Live Laugh Love Care’ which supports those seeking psychological support by linking them with mental health professionals. Such simple grassroots-driven measures reduce the burden on the public health sector.
Recent discussion has pressed for reform of the country’s mental health policy, a colonial era piece of legislation whose title, The Lunacy Act 1912, speaks volumes. This is crucial and should be a top priority for the NLD government. Thankfully, the past year has shown glimmers of hope that this message is getting through. Significant change is afoot in approaches to illicit drug control, a change that will, if carried through, have positive impacts on mental health outcomes in the country. In February, the Ministry of Home Affairs said that it was working with UNODC toward a more health-focused approach to combating illegal narcotics, rather than the previous decades-long punitive drug control approach (as displayed in Yangon’s Drug Eradication Museum). If practice matches policy laid out by the new national drug control policy, it will be a tremendous step in the right direction.
Yet despite a handful of positive steps and talk of change, concerning was the Ministry’s Public Health Statistics Report 2014-2016 released last year that had less than half a page on mental health. Of the very limited data that it did show, it failed to properly discuss a graph showing that mental retardation per 100,000 population was more than three times higher in Chin and at least six times higher in Kayah than the national average. Such a statistic on any other public health issue is unlikely to have been given such short shrift.
Again, the lack of emphasis on mental health doesn’t make economic sense. For every US$1 million invested in mental health care packages – at a cost of US$3-4 per capita – between 350-700 healthy years of life can be obtained. The argument for improving mental health in the country are clear and would have an economic windfall.
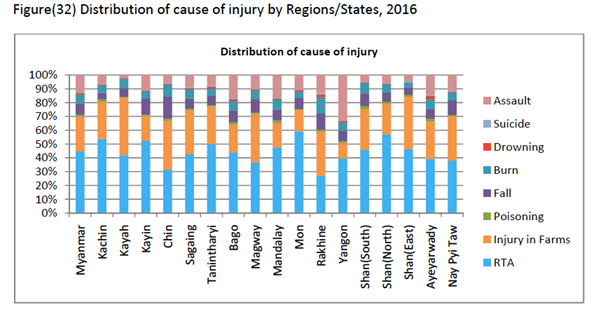
Injuries contribute a significant cause of ill-health in Myanmar. The two biggest causes of injury were Road Traffic Accidents and Injury on Farms according to the 2017 released data. The past year has seen campaigns to reduce both causes of injury. (A disturbing side statistic in the 2017 data found that assault contributed more than 30% of all causes of injury in Yangon. Unfortunately, no further analysis was given.)
Road injuries constituted 3.51% (3.04% – 4.07%) of disability adjusted life years in Myanmar in 2016, making it a significant cause of ill health. Worryingly the latest data between 2014-2016 show a steady increase – almost 10 percent annually – in road traffic accidents and related morbidity and mortality. The WHO estimate that road deaths may be as high as 20 per 100,000 population. Campaigns to improve road safety – including the wearing of seatbelts and promotion of safe tyres – improved in the past year and will go a long way to improving public health in the country. These campaigns now need to find the traction to become social norms.
The new National Health Plan 2017-2021 was launched on 31 March 2017. The document aims to strengthen the country’s health system and support the implementation of Universal Health Coverage. Central to the document is access to essential health services and reducing out of pocket costs.
In line with the document, the Ministry of Health and Sport began its roll out of the 2017 phase of its NHP in the form of essential service packages to 78 townships. Since July 2016, 10 types of vaccines have been available for free to children in Myanmar and progress has been made in improving immunization coverage, particularly for measles-rubella and of pentavalent – a combined vaccine for whooping cough, tetanus, hepatitis B, diphtheria and haemophilus influenza B. Still however in 2016 reported data, there were five townships that had no reporting – one of those was in Naga where the 2016 outbreak of measles killed dozens. If the country is going to achieve the elimination of measles by 2020, it will need to target these areas. Also in 2017, in a public health coup, a nationwide vaccination campaign began, billed as one of the largest public health interventions ever conducted in Myanmar, to vaccinate 14 million children against the deadly Japanese Encephalitis vaccine. The lifesaving campaign however hasn’t been without some controversy, with the Myanmar head of WHO and the government having to defend the vaccine.
Health worker density remained 60 percent lower than the regional average, according to 2016 data. With more people going to hospitals than ever before – in part due to improved awareness, transportation, security, and available medicines – improving capacity in the health sector will be increasingly important. Data from 2015 showed that only 43 percent of the population had access to affordable medicines and vaccines on a sustainable basis. That must improve if objectives of the NHP are to be met. Indeed, it demonstrates the work that still must be done to improve equal access to health care in Myanmar and to improve public health more generally. At the top of that list remains the appropriate and timely allocation of resources.
As an excellent and constructive critique by Ye Min Zaw noted earlier this year, the NLD government despite a commitment to reform “has wasted its resources and failed to adequately fund its health care system.” Under pressure, the Minister stated a new commitment to improve and streamline the reporting system of acquisition and distribution of medicines, which the minister said would help improve efficiency and reduce waste. However, as Ye Min Zaw notes, “the government talks more about big dreams than about attainable objectives.” That sentiment speaks volumes.
The government must realign itself to those working at the coal face of public health. In doing so, in 2018, they can better align public health objectives with public health realities and build on some of the successes of the past year.
Elliot Brennan is a Non-Resident Research Fellow at the Institute for Security and Development Policy in Stockholm. He previously worked with the Joint Ceasefire Monitoring Committee and the Myanmar Peace Centre in Yangon. Prior to these engagements he worked as a Non-Resident WSD-Handa Fellow with Pacific Forum CSIS, as the Southeast Asia Analyst for the Lowy Institute’s Interpreter and a contributing analyst at IHS Jane’s.